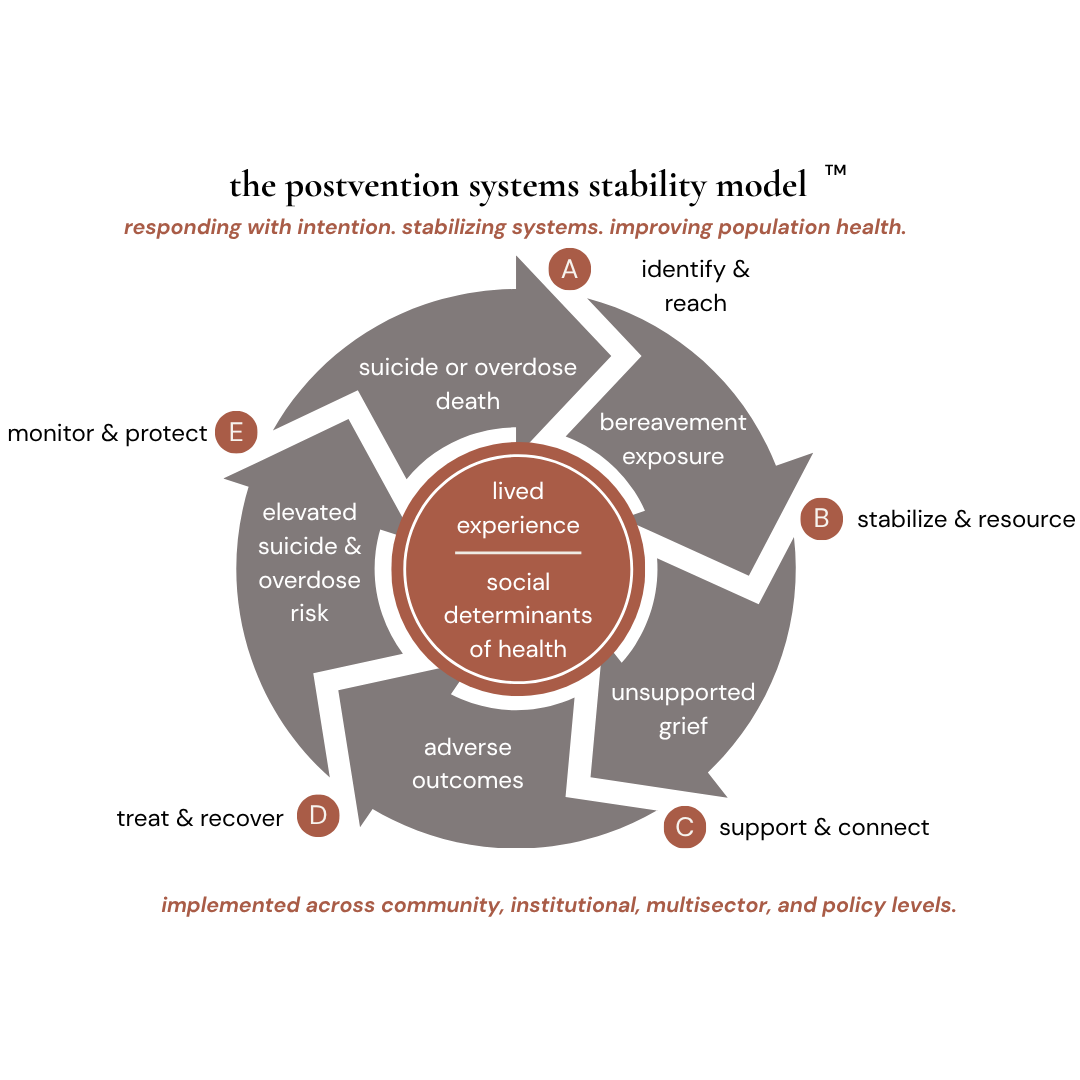
the cycle of unsupported loss
the cycle begins when a suicide or overdose death occurs, immediately exposing survivors to bereavement and its distinctive relational, psychological, and social challenges. without effective postvention, that exposure can progress into unsupported grief — often marked by isolation, stigma, and social invalidation.
over time, unsupported grief may contribute to adverse psychosocial outcomes tied to the social determinants of health, including disruptions in social support, economic stability, mental health, and family functioning. left unaddressed, these adversities can elevate future suicide and overdose risk, perpetuating the cycle across individuals, families, and communities. lived experience and the social determinants of health sit at the center as cross-cutting conditions shaping both vulnerability and access to support.
five action points that interrupt the cycle
a — identify & reach. following a death, identify direct and indirect survivors and initiate responsible, proactive outreach — reaching beyond next-of-kin
b — stabilize & resource. at bereavement exposure, reduce instability through sdoh-responsive support and coordinated access to practical resources — financial assistance, service navigation, housing, and caregiving help.
c — support & connect. at the onset of unsupported grief, activate validating, survivor-centered connection across formal and informal care, prioritizing affirming, lived-experience-informed engagement.
d — treat & recover. as adverse outcomes emerge, screen for complex grief and connect survivors to evidence-based, trauma-informed, meaning-oriented care — treating recovery as both clinical and structural.
E — monitor & protect. at the point of elevated risk, sustain long-term monitoring, continuity of care, and protective intervention — means-safety planning, harm reduction, and peer recovery support.
frequently asked questions
-
pssm is a public health implementation framework that helps communities build coordinated systems of support after suicide and overdose loss. it identifies five action points — identify & reach, stabilize & resource, support & connect, treat & recover, and monitor & protect — where coordinated systems can interrupt the cycle of unsupported bereavement. pssm is designed to be implemented across community, institutional, multisector, and policy levels.
-
most postvention efforts have evolved separately for suicide and overdose loss, even though survivors often face many of the same challenges accessing coordinated support. pssm was developed to provide one implementation framework that helps communities align and strengthen support across both.
-
supporting people after suicide and overdose loss isn't separate from prevention — it's an essential part of it. people bereaved by suicide and overdose loss face elevated risk themselves. coordinated postvention reduces isolation, strengthens connection, supports healing, and creates opportunities to identify and respond to ongoing risk.
-
pssm is implemented through a four-phase process — discover, design, build, and adapt — tailored to each community's needs, priorities, and resources. see how we work.
-
pssm is designed for communities seeking to strengthen support after suicide and overdose loss. it can be adapted across public health, healthcare, behavioral health, education, first responders, community organizations, and other settings where coordinated postvention is needed.
-
communities typically begin with a discovery phase — understanding current strengths, stakeholders, and opportunities to strengthen coordination — before co-designing an implementation plan together. start the conversation
-
the postvention project partners with communities, organizations, and cross-sector coalitions to understand their current postvention response, develop coordinated implementation plans, strengthen implementation through facilitation and technical assistance, and support continuous improvement over time — all guided by pssm.
-
because communities usually already have compassionate people, capable organizations, and valuable resources responding to loss. the challenge isn't effort — it's aligning those efforts so they function as one coordinated system, rather than leaving survivors to find their own way between them.
postvention systems stability model™ (pssm)
the postvention systems stability model™ (pssm) illustrates the self-perpetuating cycle through which unsupported bereavement contributes to additional adverse outcomes and identifies the points where that cycle can be interrupted. it reframes postvention not as a reactive response to death, but as a proactive form of prevention — a coordinated systems response rather than a clinical intervention alone. the model is implemented across community, institutional, multi-sector, and policy levels.