strengthening support for people affected by suicide and overdose loss
prevention begins with the bereaved.
the postvention project partners with communities to build coordinated postvention systems, guided by the postvention systems stability model™ (pssm).
building on what already exists
every community already has people, organizations, and relationships dedicated to supporting survivors after suicide and overdose loss.
what communities often don't have is a clear picture of how those efforts connect—or an intentional postvention system designed to support survivors across organizations and over time.
we help communities uncover opportunities to align and strengthen the systems they already have.
survivors shouldn't have to navigate the system alone
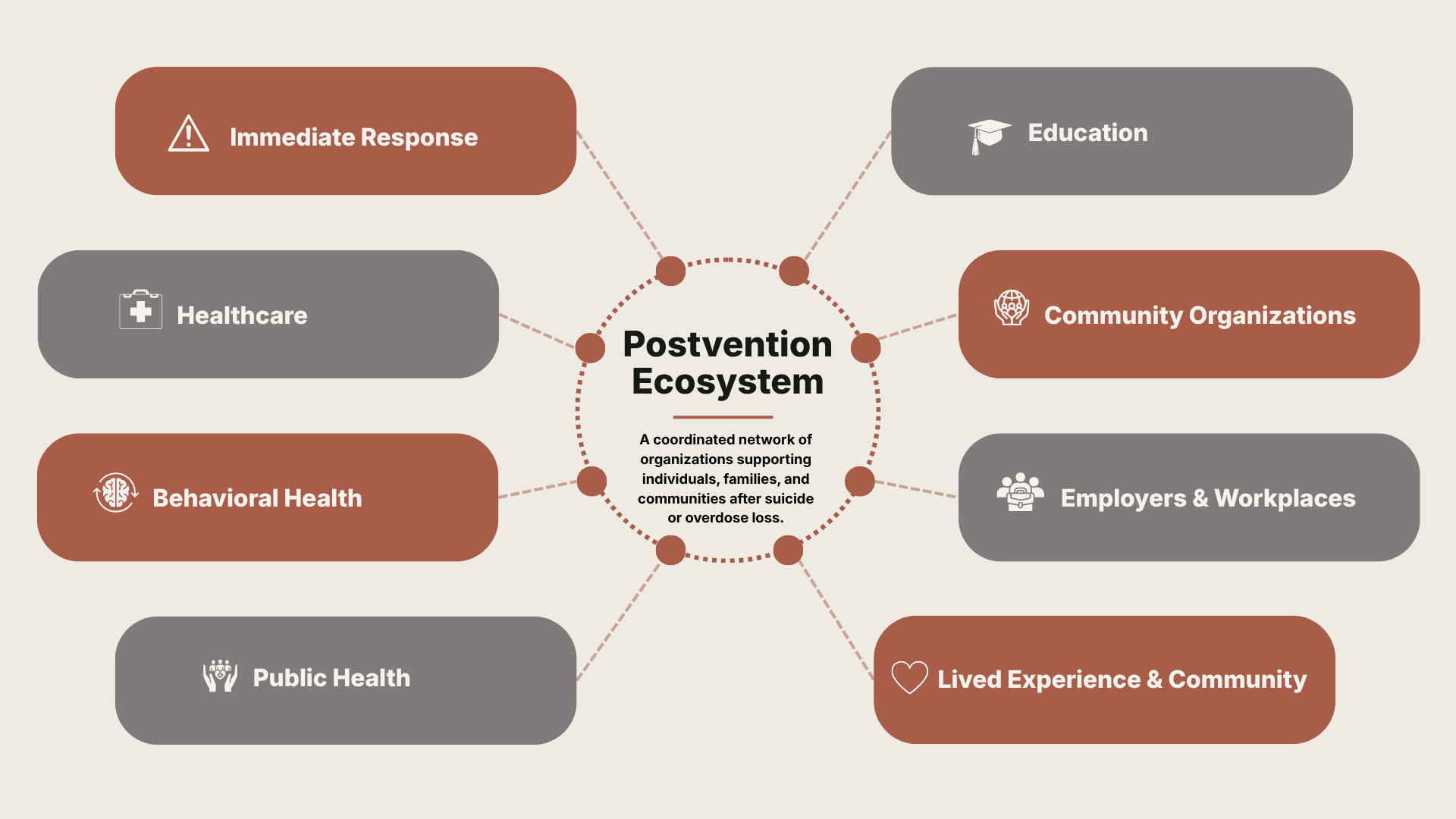
after a suicide or overdose death, supportive resources are available in most communities. but they're often spread across organizations, with resources becoming available at different points over time—rarely experienced as one coordinated system.
so, the person carrying the weight of profound grief becomes the one who has to figure out who to call, where to turn, and which resource is the right fit.
a coordinated system changes that. survivors spend less time searching for help and more time receiving the care they need after a traumatic loss.
our strongest partnerships are with leaders asking questions like...
if a community member lost someone close to them after a suicide or overdose death today, would they know where to turn?
if someone contacted us after a suicide or overdose death today, would we know who to connect them with?
where are survivors left to connect the dots on their own?
where do handoffs between organizations break down?
what would it take for survivors to experience one coordinated system of support?
if you and your collaborators are asking these questions, we'd love to work with you.
our partnership process
every partnership begins with understanding your community's current postvention response. from there, we work together to develop a coordinated implementation plan grounded in your goals, strengths, and existing partnerships.
discover
understand your current landscape.
identify existing strengths, stakeholders, and opportunities while uncovering gaps in coordination.
our partnership process is guided by the postvention systems stability model™
design
create a shared roadmap.
develop a coordinated implementation plan tailored to your community's needs, priorities, and resources.
build
put your plan into action.
support implementation through facilitation, technical assistance, and training.
adapt
strengthen your system over time.
evaluate progress, refine implementation, and support continuous learning as your community evolves.
ready to strengthen your community's response?
if you're exploring how to strengthen support after suicide or overdose loss, we'd welcome the opportunity to learn about your community and discuss how we might work together.